|
|
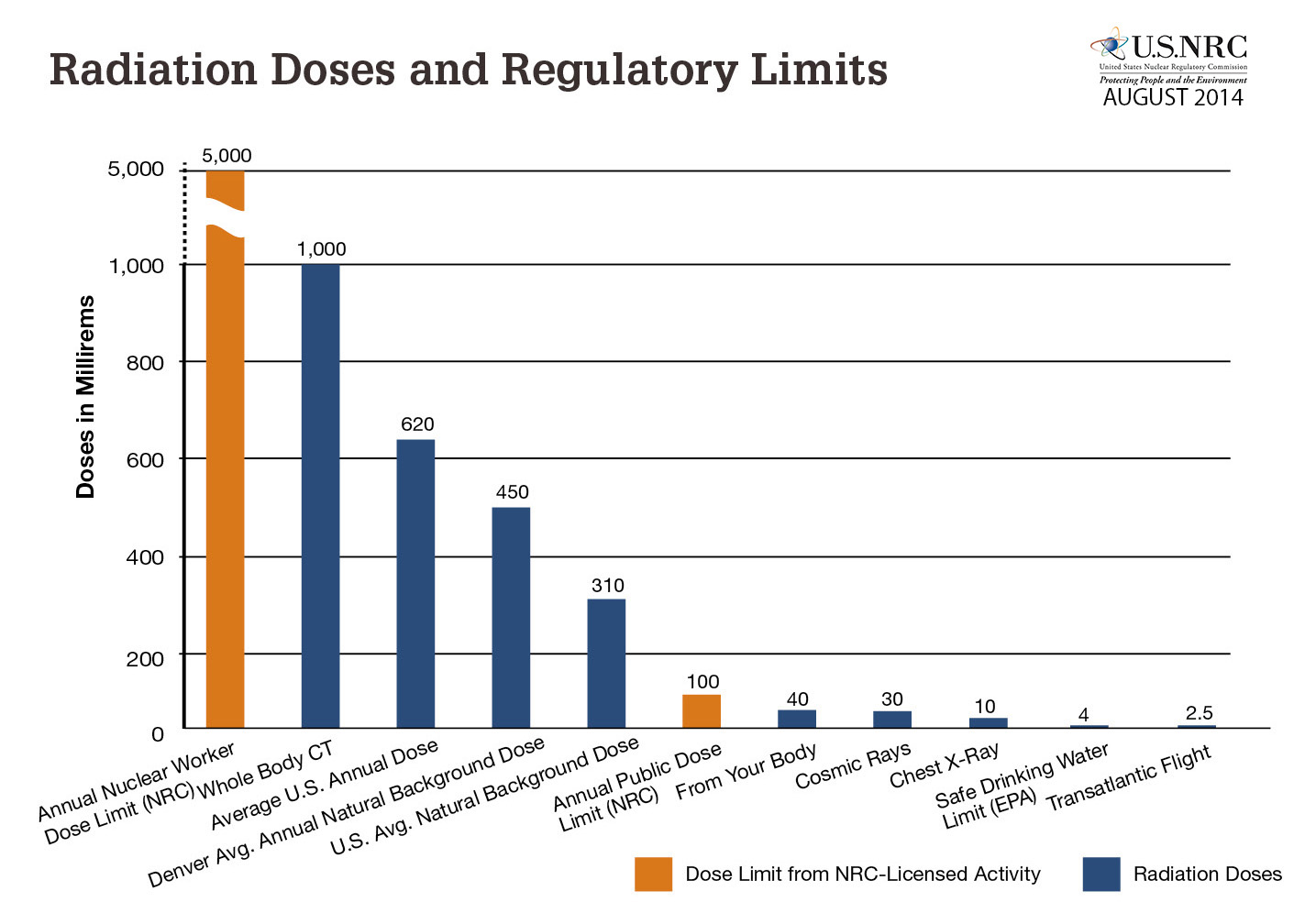
| Fig. 1: This plot compares the maximum doses to both radiation workers and the public as given in NRC regulations (orange bars) to other doses of interest. [4] (Courtesy of the NRC.) |
Not long after the discovery of ionizing radiation, it became clear that exposure to high doses of such radiation was detrimental to human health. Nowhere was this more starkly evident than after the atomic bombings of Hiroshima and Nagasaki during the second World War, when thousands of those who survived the initial blast were affected by radiation sickness, cancer, and birth defects in their future children.
After the war, as the United States moved toward further investment in both nuclear weaponry and nuclear energy for civilians, the Atomic Energy Commission (AEC), and later the Nuclear Regulatory Commission (NRC), laid out increasingly stringent safeguards to protect both civilians and nuclear workers. This effort culminated in the ALARA (As Low As Reasonably Achievable) protocol, which eventually became adopted as the gold standard of nuclear safety.
Though the conservative ALARA framework has been largely successful in preventing occupational and accidental civilian exposure to ionizing radiation, it has not come without economic cost. We will review the scientific evidence behind ALARA and potential alternatives. Within our current understanding, ALARA correctly errs on the side of caution than of excess risk; more research to determine the true risk of low doses of ionizing radiation is necessary to determine an ideal paradigm for radiation protection.
After the discovery of ionizing radiation in the 1890s, it didn't take long for researchers to notice its deleterious health effects. It became known anecdotally within the scientific community that sufficient exposure could lead to problems from skin rashes and hair loss to more significant symptoms like cancer and sterility. [1] By the 1920s, it was known that exposure to ionizing radiation could lead to genetic mutations, further heightening concern about the biological effects of radiation. [2] Knowledge of these risks, along with almost all other pre-war nuclear knowledge, remained confined to the scientific community, even after the dropping of the atomic bomb. In 1954, when civilian nuclear applications were authorized and put under the control of the AEC, the benefits of nuclear energy to society were widely broadcast, while safety issues were considered an internal matter. [1]
The AEC had a dual remit to promote as well as regulate civilian nuclear energy. Though the AEC did implement safety regulations, its work was initially weighted toward promotion, in part because of the widely-hyped benefits of nuclear technology. In 1955, AEC Commissioner Willard Libby stated: "Our great hazard is that this great benefit to mankind will be killed aborning by unnecessary regulation." [1]
As public understanding of the safety risks of nuclear energy increased, demand for stricter regulations on radiation exposure and control of radioactive material rose. In the late 1950s, public debate raged over the danger of fallout from nuclear testing. In response, the AEC tightened its dose limits in 1961. [1] Later in the 60s, concern flared up again over public radiation exposure from routine operation of nuclear power plants. Again, to pacify public criticism, the AEC tightened limits of releases of radioactive material from power plants. [1]
Because of this public outcry over safety and several high-profile regulatory missteps, the AEC was an embattled agency by the early 1970s. "The competing responsibilities and the precedence that the AEC gave to its military and promotional duties gradually damaged its credibility on regulatory issues and undermined public confidence in its safety programs." [1] In response, the AEC was divorced into two agencies in 1974, with promotional duties handled by an agency that later became the cabinet-level Department of Energy (DOE) and regulatory power given to the NRC, which deals with nuclear safety and licensing issues to this day. The current NRC maximum yearly dose limits for radiation workers and the general public are shown in Fig. 1.
The decisions by the AEC to make radiation protection regulations increasingly strict were motivated more by public outcry than by scientific investigation. Little was known at the time about the true health effects (or lack thereof) of low doses of radiation, but the public rhetoric was often stinging. Vocal critic John Gofman wrote, "the AEC is [hoping] that the benefits [of nuclear energy] outweigh the number of deaths...This is legalized murder, the only question is how many murders." [1] It is in this context that our modern radiation protection protocol, ALARA, was born.
Since 1974, radiation protection regulations have been created and enforced on a federal level by the NRC. The regulations established the safety protocol known as ALARA, which is defined as:
"Making every reasonable effort to maintain exposures to radiation as far below the dose limits in this part as is practical consistent with the purpose for which the licensed activity is undertaken, taking into account the state of technology, the economics of improvements in relation to state of technology, the economics of improvements in relation to benefits to the public health and safety, and other societal and socioeconomic considerations, and in relation to utilization of nuclear energy and licensed materials in the public interest." [3]
This protocol comes on top of the maximum permissible dose restrictions shown in Fig. 1. The result of the ALARA requirement is that although these maximum doses are rather high (50 mSv per year for radiation workers), the ALARA protocol results in actual radiation worker doses (shown in Fig. 2) that are much lower. Among workers who received a measurable dose of radiation, the average yearly dose is 1mSv per worker, which is approximately the maximum dose limit for a member of the general public. [4]
Of course, even with a low average dose among measurably exposed workers, it may happen that many workers receive low doses while a few experience very high, potentially dangerous levels of exposure. While the average dose among workers with measurable exposure is not an exact proxy for overall safety, it is the statistic "most commonly used in [NRC] and other reports when examining trends and comparing doses received by individuals in various segments of the nuclear industry." [5] In spite of its shortcomings, the NRC uses it as evidence for the success of ALARA: "The overall decreasing trend in average reactor collective doses since 1994 indicates that licensees are continuing to successfully implement as low as is reasonably achievable (ALARA) dose reduction processes at their facilities." [5]
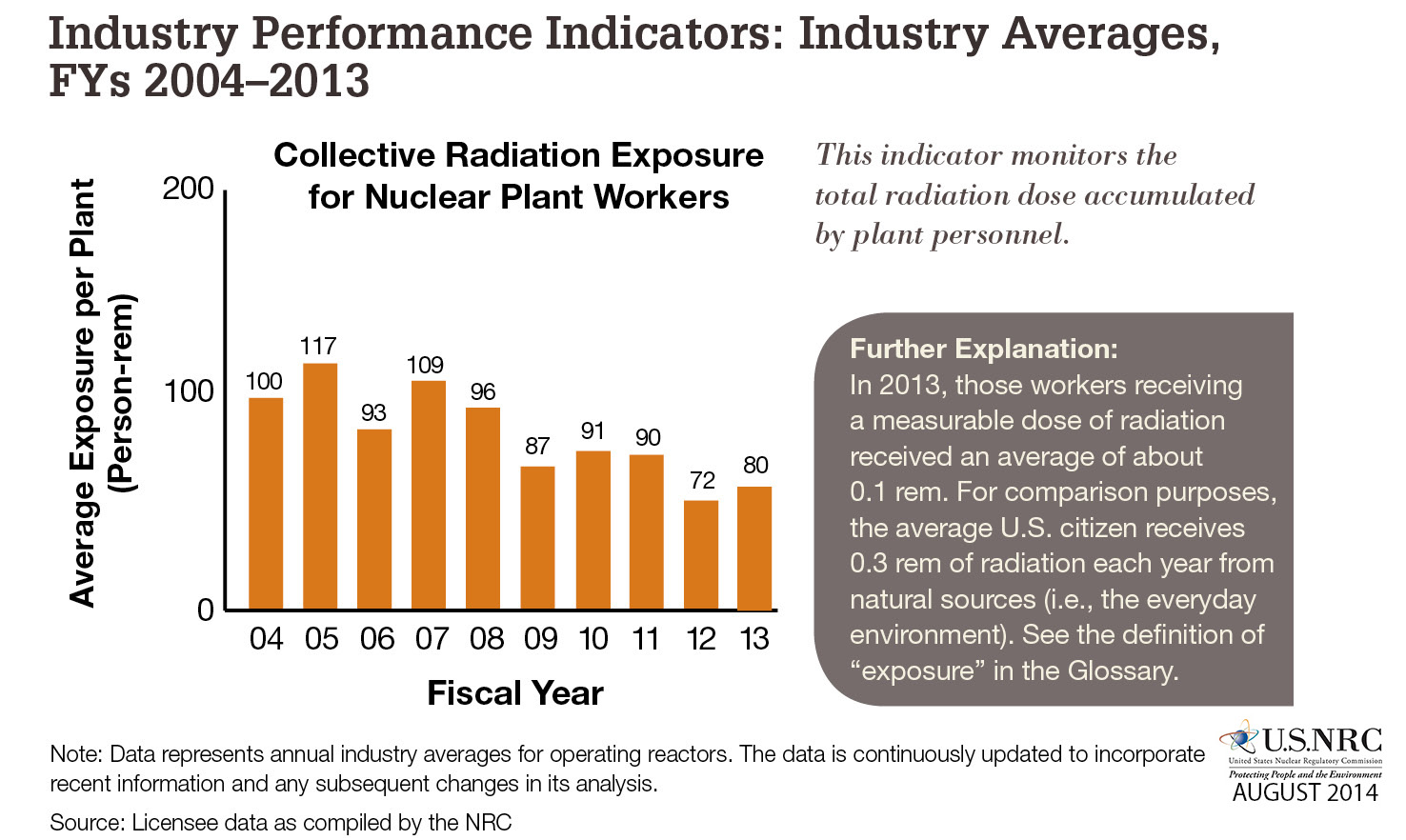 |
| Fig. 2: This plot shows the actual, cumulative dose absorbed by radiation workers in the US from 2004-2013. [4] These data correspond to an average dose per worker of only 1 millisievert, much less than is required by NRC regulations. (Courtesy of the NRC.) |
The principle of ALARA, which results in actual doses far below the maximum permitted, is consistent with the most recent (2006) report from the National Research Council, which holds that "there is no compelling evidence to indicate a dose threshold below which the risk of tumor induction is zero." [6] The report does admit, however, that "at doses less than 40 times the average yearly background exposure (100 mSv), statistical limitations make it difficult to evaluate cancer risk in humans", leaving the relationship between dose and response (health outcome) an open question below 100 mSv. [6] If low doses of radiation were shown to be sufficiently safe, the ALARA protocol might be able to be relaxed, increasing the efficiency of and potential investment in the nuclear industry. In the following section, we explore various concepts in health physics that offer potential answers to this difficult but important unsolved question.
Although the ALARA protocol has ostensibly been a success - a large study showed no increased risk of cancer in US counties that are home to nuclear power plants [6] - some have questioned whether the protocol is too conservative, imposing unnecessary costs on the nuclear industry and society at large.
By its nature, ALARA demands only measures that are "reasonably achievable" be implemented to reduce radiation exposure; however, the definition of what is "reasonable" is unclear. If it is true that there is no dose level of radiation without additional risk, then significant costs are incurred in reducing risk to the lowest level possible: "when risks are small to begin with, further reductions become increasingly difficult to achieve, and increasingly more resources must be applied." [7]
Given that the relationship of dose and outcome below 100 mSv is unclear, some have proposed replacing ALARA with a less conservative protocol. Wade Allison, an Oxford professor who regularly argues for relaxed radiation restrictions, claims that not only would this reduce operational compliance costs at nuclear facilities, but it would also prevent regulatory overreaction during nuclear emergencies. [8]
Nuclear disasters like the recent Fukushima Daiichi incident illustrate vividly the unavoidable economic and social costs of nuclear exposure: people are forced to evacuate their homes (some for the long-term), food and goods are condemned as contaminated, and victims can experience both physical and mental health problems. [9] Some of these costs are unavoidable, while others depend on the dose limits that are deemed acceptable. If acceptable limits can reasonably be set higher, then less land and fewer resources need be condemned in the wake of disaster. As Jim Smith argues:
"The long-term response to Fukushima will have to be pragmatic. The Japanese authorities may have to rewrite the rule-book, as they have begun to do in allowing doses of 250 mSv for radiation workers. After an accident, it may be appropriate to set exposure limits for members of the public higher than the typical 1 mSv per year maximum. A limit of 5-10 mSv per year (perhaps with voluntary resettlement at doses above 1 mSv per year) may be appropriate, bearing in mind that millions of people in areas of high natural radioactivity worldwide are exposed to more than 10 mSv per year, and that occupational exposures (for example, to long- haul air crews) can be around 5 mSv per year." [9]
Allison concurs, saying that "public authorities react by providing over-cautious guidance - and this simply escalates public concern." [8] After the Chernobyl disaster, he notes, Swedish authorities admitted to setting safety levels over-cautiously, resulting in the unnecessary condemnation of large amounts of meat. [8]
Prof. Allison goes even further by advocating for an overall change in radiation safety paradigm: instead of ALARA, he suggests AHARS (As High as Relatively Safe). [8] This thinking is based on the idea that doses below a certain threshold are essentially harmless, and therefore don't merit the strict and costly limitations of ALARA, but evidence for this hypothesis is inconclusive. [6] We discuss the health physics underlying ALARA and alternative protocols in the following section.
 |
| Fig. 3: While data from atomic bomb survivors constrain the dose-response relationship to be linear above doses of 100 mSv, the dose-response relationship at lower doses is not precisely known. The LNT model (A), which is the basis of the ALARA protocol, is the most conservative, while other models with sub-linear (B) or thresholded (C) response have also been proposed. (After USNRC NUREG-0713. [5]) |
As discussed in Section 2, radiation protection protocol has historically been made increasingly strict due to public backlash, but as Kenneth Mossman notes, "The public's views of risk do not necessarily coincide with reality." [7] In this section, we discuss the current state of scientific understanding of the health effects of radiation, particularly at low doses.
Data from survivors of the atomic bombings can shed light on the dose-response relationship, particularly at high dose levels, as people who were close to the hypocenter at the time of the detonation received severe doses of radiation. By estimating received dose based on distance from the hypocenter and following survivors for many years after the bombing, Douple et al. showed a linear relationship between received dose and cancer risk for doses above 100 mSv. [10]
Below doses of 100 mSv, uncertainties in actual absorbed dose become quite large, and the contribution of risk from spontaneous (i.e. from causes other than radiation exposure) cancer becomes an important factor. [11] On top of that, biological repair mechanisms have the potential to repair the damage done to cells by ionizing radiation, thus at least somewhat mitigating cancer risk from exposure at low dose levels. [12]
Various models of the relationship between dose and response have therefore been proposed. [6] The linear-no-threshold (LNT) model, labeled "A" in Fig. 3, is the model that is the basis of the ALARA protocol; if even small doses lead to slight increases in risk of cancer, than doses should be kept as low as possible. Other models ("C" in Fig. 3) propose a threshold below which low doses do not lead to increased risk of cancer. This as well as sub-linear response models ("B") are often based on the idea biological repair mechanisms reduce or eliminate the risk of cancer at low doses. [12]
Ultimately, however, the evidence thus far is inconclusive, and given the scope of the risks at stake, ALARA is a reasonable choice as a conservative safety protocol, at least until further research illuminates the true risk of low doses of radiation to human health. The DOE has had a low-dose research program active since the late 1990s. Although it "has seen its funding and visibility decline since it was first created," as of January 2015, renewed Congressional interest offers the potential of an increase in future research in this area. [13]
Despite its genesis in public opinion rather than scientific investigation, the ALARA protocol has successfully limited the exposure of radiation workers to impressively low levels of around 1 mSv. The grounding of ALARA is in the linear-no-threshold hypothesis, which states that risk is directly proportional to dose, even for the smallest exposures. Although significant costs are incurred to conform to ALARA and the validity of the LNT model is unclear below doses of 100 mSv, more research on the health effects of low radiation doses is necessary before alternatives to ALARA can become viable.
© Michael Baumer. The author grants permission to copy, distribute and display this work in unaltered form, with attribution to the author, for noncommercial purposes only. All other rights, including commercial rights, are reserved to the author.
[1] J. S. Walker and T. R. Wellock, "A Short History of Nuclear Regulation, 1946-2009," US Nuclear Regulatory Commission NUREG/BR-0175, October 2010.
[2] R. J Preston, "Radiation Biology: Concepts for Radiation Protection," Health Phys. 88, 545 (2005).
[3] "Standards For Protection Against Radiation, U.S. Code of Federal Regulations, 2014 Ed., 10 CFR 20, 1 Jan 14.
[4] "2014-2015 Information Digest," U.S. Nuclear Regulatory Commission, NUREG-1350, Vol. 26, August 2014.
[5] "Occupational Radiation Exposure at Commercial Nuclear Power Reactors and Other Facilities 2012," US Nuclear Regulatory Commission NUREG-0713, Vol. 34, April 2014.
[6] Health Risks from Exposure to Low Levels of Ionizing Radiation (National Academies Press,2006).
[7] K. L. Mossman, Radiation Risks in Perspective (CRC Press, 2006).
[8] W. Allison, "We Should Stop Running Away From Radiation," BBC News, 26 Mar 011.
[9] J. Smith, "A Long Shadow over Fukushima," Nature 472, 7 (2011).
[10] E. V. Douple et al., "Long-term Radiation-Related Health Effects in a Unique Human Population: Lessons Learned from the Atomic Bomb Survivors of Hiroshima and Nagasaki," Disaster Med Public Health Prep. 5 S122 (2011).
[11] D. Billen, "Spontaneous DNA Damage and Its Significance for the 'Negligible Dose' Controversy in Radiation Protection," Radiat. Res. 124, 242 (1990).
[12] T. Neumaier et al., "Evidence For Formation of DNA Repair Centers and Dose-Response Nonlinearity in Human Cells," Proc. Nat. Acad. Sci. (USA) 109, 443 (2012).
[13] "Low-Dose Radiation Research Act of 2014," Congressional Record 160, No. 140, H8011, 17 Nov 14.