|
|
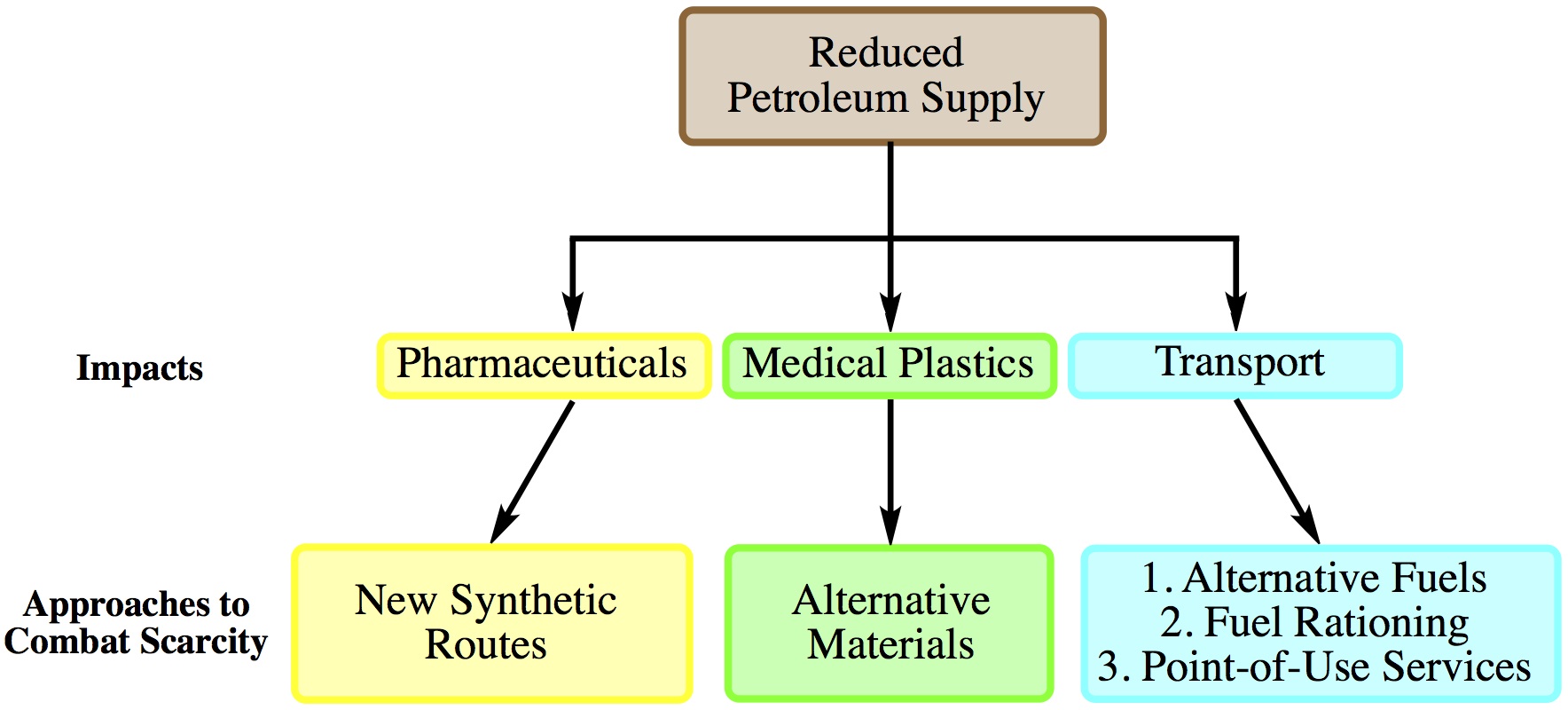
| Fig. 1: Impacts of petroleum scarcity on health care and possible policies to combat these effects. |
Petroleum is the preeminent energy source in the US and throughout the world. It has countless uses, ranging from transportation to electricity generation to crayon production.
The idea of peak oil is not new, first proposed by M. King Hubbert in 1956. [1] In summary, petroleum is a finite resource and peak oil is the point in time corresponding to the maximum rate of petroleum extraction. Although the impact of and solutions to declining petroleum supplies have been examined at great length, discussion of the effects on health care has been limited.
Awareness of the dependence of health care on petroleum became apparent following the 1973 oil embargo. Though a number of papers were published during the 1970s and 80s, much of the public attention to this issue has since faded. Nevertheless, the health care sector continues to be fundamentally dependent upon petroleum. If petroleum reserves dried up tomorrow, the provision of pharmaceuticals, medical plastics, and healthcare personnel and patient transport would be greatly affected.
While there is no comprehensive review on the petrochemical inputs in chemical therapeutics, this input is significant. The petroleum inputs in pharmaceutical drugs represent a small fraction of total petroleum use, however, petrochemical based precursors are used to make countless therapeutics. While alternative chemical syntheses often exist to generate a given compound, adoption of one of these syntheses can increase manufacturing costs. Patients will absorb not only these increased production costs, but also the costs associated with Food and Drug Administration approval of the alternative syntheses.
There has been a transition from reusable metal, glass, or rubber medical devices to inexpensive single-use, disposable plastic ones since the 1980s, in large part due to the emergence of HIV. [2] Medical devices are now critically dependent upon processed plastics derived from oil. Gloves, bags, syringes, tubing, infusion sets, and heart valves are a few of the plastic-based supplies and devices that are important in medical life support. [3] The availability of these plastic devices has become linked to high quality medical care, and thus patient health.
The US transportation infrastructure is built almost exclusively around fossil fuels. As a result, transportation for patients, staff, services, and supplies is heavily petroleum dependent. For example, ambulances and medevac helicopters bring sick or injured patients to hospitals; cars and buses bring most patients to their appointments and health care providers to work; trucks deliver food, medical devices, and cleaning supplies to hospitals. Transportation of staff requires the most significant use of petroleum, estimated to be 3.8 million gallons of gasoline annually stemming from 7.2 billion trips per year. [4] The estimate for trips made by patients is lower than for staff though it is still large, likely around 2.2 billion trips per year. [5] While the total transportation costs of supplies and services are unknown, the importance of petroleum to transport patients, staff, and supplies cannot be overstated.
Petroleum scarcity would impact heath care provision in ways not discussed above. For example, combustion of petroleum is used to provide electricity to and heat for medical facilities. While the majority of this heat and electricity comes from combustion of coal and natural gas, these sources are also fossil fuels that will have their own supply problems in the future.
Petroleum reserves will not dry up tomorrow, but how long will they last? 100 years? 500 years? While uncertainty regarding absolute petroleum reserves makes this estimate difficult, a decline in petroleum production is likely in the 21st century. Preparation for this decline is essential for maintaining our current standard of health care.
Petroleum supply shocks provide another challenge facing the health care sector. In the past, during the 1973 oil embargo, shortages in benzene and ethylene resulted in elevated prices for and delayed delivery of plastic-based medical equipment. [3] Policies must be adopted to make the health care sector more resilient to these supply shocks.
New technologies will be critical for maintaining our current standard of health care. Biofuels, bio-plastics, and electric vehicles already exist, and will undoubtedly help mitigate the effects of reduced petroleum supplies. But will these technologies be able to replace all petroleum-based products in their current states?
The answer to this question is also uncertain. In the absence of technological advancement, there is a significant chance that these technologies will be unable to replace all materials that rely upon petroleum. As a result, planning efforts must also generate policies to address future petroleum scarcity. These policies could include: [6,7]
Developing new synthetic routes to generate pharmaceuticals that limit or eliminate use of petroleum inputs.
Identifying supplies and equipment vulnerable to shortages, and appropriate alternatives such as glass instead of plastic supplies.
Adopting plans to ration fuels to emergency medical transport.
Distributing some health care services to the points of use.
This list is far from comprehensive, and others have developed more extensive plans. [3,4,6-8]
Dependency of the health care sector on petroleum makes it particularly susceptible to supply shifts. While the task of reducing the health care sector's dependence on petroleum will be difficult, it will be essential for maintaining health care provision in the face of future petroleum scarcity.
© Nicholas Plugis. The author grants permission to copy, distribute and display this work in unaltered form, with attribution to the author, for noncommercial purposes only. All other rights, including commercial rights, are reserved to the author.
[1] M. K. Hubbert, "Nuclear Energy and the Fossil Fuels," Shell Development Company, Publication No. 95, June 1956.
[2] I. Chen, "In a World of Throwaways, Making a Dent in Medical Waste," New York Times, 5 Jul 10.
[3] G. B. Clark and B. Kline, "Impact of Oil Shortage on Plastic Medical Supplies," Public Health Rep. 96, 111 (1981).
[4] J. Hess et al., "Petroleum and Health Care: Evaluating and Managing Health Care's Vulnerability to Petroleum Supply Shifts," Am. J. Public Health 101, 1568 (2011).
[5] S. M. Schappert and E. A. Rechtsteiner, "Ambulatory Medical Care Utilization Estimates for 2006," Natl. Health Stat. Reports, No. 6, 6 Aug 08.
[6] A. E. Raffle, "Oil, Health, and Health Care," Brit. Med. J. 341, 617 (2010).
[7] H. Frumkin, J. Hess and S. Vindigni, "Peak Petroleum and Public Health," J. Am. Med. Assn. 298, 1688 (2007).
[8] A. B. Kline, "Will Shortages of Raw Materials and Rising Prices Hurt Our Chances for Better Health Care?," Public Health Rep. 90, 3 (1975).